Case Report
Brock P1, Nasur R2, Deshpande S1, Ellis R3, and Al-Inizi S2*
1Department of Anaesthesiology, South Tyneside NHS Foundation Trust, South Shields, UK
2Departments of Obstetrics & Gynaecology, South Tyneside NHS Foundation Trust, South Shields, UK
3Department of Microbiology, South Tyneside NHS Foundation Trust, South Shields, UK
Corresponding author
Dr. Shamma Al-Inizi, Consultant Obstetrician and Gynaecologist, South Tyneside NHS Foundation Trust, Harton Lane, South Shields, UK, Tel: +441914041000/Ext: 4018; E-mail: shamma.al-inizi@stft.nhs.uk
Received Date: 01st June 2015
Accepted Date: 20th June 2015
Published Date: 25th June 2015
Citation
Al-Inizi S (2015) Adult Onset Still?s Disease Complicated by Chlamydia pneumoniae in Pregnancy. Enliven: Gynecol Obstet 2(3): 004.
Copyright
@ 2015 Dr. Shamma Al-Inizi. This is an Open Access article published and distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Adult onset Still’s disease in pregnancy (AOSD) is a rarely made diagnosis- in this case it emerged from a presentation complicated by Chlamydia
pneumoniae and did a fair job in mimicking a much more common obstetric syndrome of HELLP (Haemolysis, Elevated Liver enzymes, Low platelets)
syndrome. Case reports have associated pregnancy, Chlamydia infection and AOSD, but both in combination together with thrombocytopenia appear to
be unique to the literature.
Keywords
Stills disease; Pregnancy; Chlamydia; Thrombocytopenia
Abstract
Adult onset Still’s disease in pregnancy (AOSD) is a rarely made diagnosis- in this case it emerged from a presentation complicated by Chlamydia pneumoniae and did a fair job in mimicking a much more common obstetric syndrome of HELLP (Haemolysis, Elevated Liver enzymes, Low platelets) syndrome. Case reports have associated pregnancy, Chlamydia infection and AOSD, but both in combination together with thrombocytopenia appear to be unique to the literature.
Case Presentation
A 33 year primigravada presented at 30 weeks plus 6 days gestation to the medical assessment unit at a district general hospital. She described a fluctuating fever, cough and a rash on her upper thighs, back and buttocks for the past 5 days.
Previous to this she had an uncomplicated, low risk pregnancy with normal antenatal booking blood tests and scans. She had no significant past medical or family history.
Examination confirmed a macular rash on her back (Figure 1) and found cervical lymphadenopathy, oral thrush, signs of dehydration and decreased air entry at both lung bases. She was hypotensive, tachycardic and febrile.

Figure 1: Salmon coulored macular rash on the back
Initial blood tests are detailed in (Table 1). She was anaemic, with low platelets, raised inflammatory markers and deranged liver function tests. Her chest x-ray was reported as clear and urine analysis showed ketones ++ and protein +. Fetal scan showed a breech presentation, normal liquor volume with an anterior placenta that was not low.
|
Hb |
10.2 |
12.8 |
12 |
12.6 |
12.3 |
12.6 |
12.8 |
12.5 |
|
Platelets |
63 |
56 |
58 |
62 |
60 |
99 |
167 |
180 |
|
WBC |
10.000 |
11.000 |
8.6000 |
8.4000 |
|
9.0000 |
|
|
|
ALT |
89 |
76 |
54 |
66 |
|
89 |
98 |
490 |
|
AP |
143 |
159 |
191 |
220 |
280 |
320 |
390 |
498 |
|
CRP |
213 |
201 |
|
230 |
303 |
301 |
303 |
334 |
|
lactate |
|
4.01 |
|
|
|
|
|
|
Table 1: Blood investigations from day 1-day 13 (AP: Alkaline phosphatase, Hb: Haemoglobin, ALT: alanine aminotransferase)
On review by the consultant physician, obstetrician and anaesthetist, a provisional diagnosis of HELLP syndrome and sepsis of unknown source was made. Repeat blood tests showed the abnormalities to be worsening with more severe thrombocytopenia (Table 1). She was given a stat dose of cefuroxime on microbiological advice and was taken for a category II Caesarean section (CS) under general anaesthetic after discussing her case with haematology and paediatric colleagues. Two units of blood and one pool of platelets were prepared and given to the patient accordingly.
An uneventful CS resulted in the delivery of a healthy female baby of 1930g with an Apgar score of 9/9. After two weeks stay on the special care baby unit, she was discharged home.
The mother had no pus in the peritoneal cavity and a normal appendix on visualisation with no other intraoperative focus for infection identified. Post procedure as she remained hypotensive, with repeated attacks of desaturation, an arterial line was inserted and was transferred to the intensive care unit for inotropic support. She was commenced on meropenem and metronidazole upon microbiologist advice as she continued to be pyrexial at 38.2ºC. She remained ventilated and was extubated 24 hours later. A chest X-Ray after 24 hours on the unit showed right basal consolidation with pleural effusion (Figure 2) and it was thought that the source of the sepsis had been found.
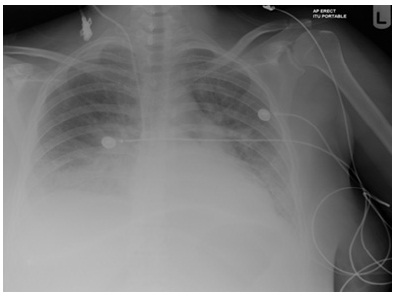
Figure 2: Chest x ray showing right sided basal consolidation& pleural effusion
With baby delivered and the source of sepsis seeming clear a smooth recovery was anticipated. Unfortunately, over the next three days her rash persisted, she continued to be pyrexial and she remained tachycardic. A battery of investigations was performed and is detailed in (Table 2). Of note, she had a CT thorax/abdomen which showed 14cm splenomegaly, patchy lung consolidation and bilateral pleural effusions with no abdominal collection. Her Chlamydia pneumoniae IgG was positive at a titre of 1:256 and she was commenced on clarithromycin for presumed Chlamydia pneumonia pneumonia.
|
Investigations performed |
|
Urine culture negative |
Table 2: Investigations performed
Haemodynamic ally stable, she was transferred to the medical ward. Upto day 12 of her admission her high grade fever persisted and despite antibiotics and systemic antifungal treatment, her liver function tests and inflammatory markers worsened. A full body MRI added only that the splenomegaly persisted and that the chest consolidation was resolving.
She was transferred to a specialist infectious diseases unit where further investigations were performed as detailed in (Table 2). It was day 13 of her admission when she was reviewed by a consultant rheumatologist that the diagnosis of Adult Onset Still’s Disease (AOSD) was raised. A repeat echocardiogram revealed a pericardial effusion, repeat CT abdomen showed persisting splenomegaly and a ferritin level of 16000 was found.
With the diagnosis clinically confirmed, her antibiotics were stopped and she was commenced on intravenous steroids. Happily a rapid clinical improvement was seen. She was transferred to the care of the rheumatology team and managed with oral steroids and cyclosporine.
While her inpatient stay was a long one, ultimately requiring a further 2 months in hospital, outpatient follow up at 3, 4 and 5 months post admission showed her to be well with only some residual Cushingnoid appearance as a side effect of steroids.
Discussion
Still's disease is named after English physician Sir George Frederic Still (1861-1941), England`s first professor in paediatrics.
Adult Onset Still`s Disease (AOSD) first described by By Waters in 1971, is a rare systemic inflammatory disorder of unknown aetiology [1]. However; a matched case- controlled study of 60 patients with AOSD had suggested that physical and psychological stress could be a potentially important risk factor for the disease [2]. It is a clinical diagnosis, characterised by pyrexia, arthritis, skin rashes and involvement of various organs [3]. A variety of diagnostic criteria [5] are available the most sensitive thought to be the Yamaguchi criteria [4,6,7] (Table 3).
|
Major criteria |
Minor criteria |
|
Fever of at least 39C for at least one week |
Sore throat |
|
Arthralgia or arthritis for at least two weeks |
Hepatomegaly or splenomegaly |
|
Nonpruritic salmon colored rash (usually over trunk or extremities while febrile) |
Lymphadenopathy |
|
Leukocytosis (10,000/microL or greater), with granulocyte predominance |
Abnormal liver function tests |
|
|
Negative test for ANA& RF |
Table 3: Yamaguchi criteria for AOSD
Diagnosis requires five features with atleast two being major criteria. Those highlighted in bold (Table 2) were to be found in this case, yet the diagnosis took time and expertise to come to AOSD is rare and has been described all over the world. Prevalence is estimated at 1.5 cases per 100,000 population. Treatment is by anti-inflammatory drugs and by steroids for severe symptoms. Other medications like cyclophosphamide and methotrexate have been also described as efficacious [5].
AOSD can present for the first time during pregnancy. It is a diagnosis of exclusion with nonspecific laboratory results. It has been reported that good maternal and fetal outcomes can be expected after initial diagnosis and treatment [4]. AOSD in pregnancy can be confused with many other diseases, but its diagnosis, after exclusion of other infectious, malignant, and rheumatic conditions, can portend good maternal and fetal outcomes.
Gerfaud-Valentin et al. has recently reported that AOSD in pregnancy can be responsible for obstetrical complications such as premature births. However; for patients with known AOSD, the second trimester and postpartum appear to be periods exposing to disease recurrence [8]. Thus they recommend close multidisciplinary monitoring by a rheumatologist and an obstetrician prior to, during and after pregnancies. Polyserositis in pregnancy with AOSD was reported suggesting no infectious agent could be detected and no improvement was seen after antibiotic therapy [9,10]. In this case, pleural and pericardial effusions were detected by imaging. However; anti-chlamydial therapy was continued due to the confirmation of Chlamydia pneumonia pneumonia and resolving lung consolidation on chest X ray before making the diagnosis of AOSD.
It has been reported that Adult Onset Still's disease may be triggered by certain infections, such as the Coxsackie, Parvo B19, Rubella, Mumps, Epstein-Barr, and Cytomegalo virus, as well as Mycoplasma pneumoniae, Toxoplasma gondii and Chlamydia spp. [11]. Takeda et al. reported a case of AOSD in a man with raised Chlamydia pneumonia serology Ig Gtitre which decreased slowly after the beginning of steroid therapy associated with improvement of clinical symptoms. They concluded that Chlamydia pneumoniae stress protein HSP60 could have served as the antigen to produce various cytokines leading to the establishment of the pathogenesis of the disease. They also suggested further studies to define this association between Chlamydia pneumonia pneumonia and AOSD.
Thrombotic microangiopathy and thrombocytopenia in AOSD was reported to be very rare and whether it was a coincidental finding or both diseases share a similar pathogenic mechanism was unclear [11]. In this case, progressive thrombocytopenia and elevated liver enzymes were initially thought to be due to HELLP syndrome, however; there was no evidence of pre eclampsia as a main associated factor with HELLP syndrome [12]. The acute presentation of a clinical picture mimicking severe sepsis progressing into septic shock requiring inotropic therapy and ventilation made resuscitation with multidisciplinary input and delivery of the baby highly necessary.
This picture together with thrombocytopenia, absence of arthralgia and polyarthritis resulted in the delayed diagnosis of such a rare condition.
This is the first reported case of AOSD in pregnancy complicated by Chlamydia pneumoniae pneumonia and thrombocytopenia [13].
Conclusion
Adult Onset Stills disease in pregnancy is very rare and can present in a way mimicking acute severe sepsis together with thrombocytopenia. Chlamydia Penumonia can be one of the infectious agents which triggers this disease in pregnancy. High index of suspicion together with early senior and multidisciplinary involvement in such complex rare cases in pregnancy is paramount to achieve a favourable outcome.
References
- Dunn PM (2006) Sir Frederic Still (1868-1941): the father of British paediatrics. Arch Dis Child Fetal Neonatal Ed 91: F308-F310.
- Bywaters EG (1971) Still’s disease in adult. Ann Rheum Dis 30: 121-133.
- Sampalis JS, Medsger TA Jr, Fries JF, Yeadon C, Senécal JL, et al. (1996) Risk factors for adult still`s disease. J Rheumatol 23: 2049-2054.
- Louthrenoo W, Aramsareewong T, Sukitawut W (2001) Adult onset still’s disease: clinical features and outcome in 16 Thai patients. J Clin Rheumatol 7: 301-307.
- Masson C, Le Loet X, Liote F, Dubost JJ, Boissier MC, et al. (1996) Comparative study of 6 types of criteria in adult Still's disease. J Rheumatol 23: 495-497.
- Yamaguchi M, Ohta A, Tsunematsu T, Kasukawa R, Mizushima Y, et al. (1992) Preliminary criteria for classification of adult Still's disease. J Rheumatol 19: 424-430.
- Antoniou KM, Margaritopoulos GA, Giannarakis I, Choulaki C, Fountoulakis N, et al. (2013) Adult Onset Still's Disease: A Case Report with a Rare Clinical Manifestation and Pathophysiological Correlations. Case Rep Med 2013: 981232.
- Pan VL, Haruyama, AZ, Guberman, C, Kitridou, RC, Wing DA (2003) Newly Diagnosed Adult-Onset Still Disease in Pregnancy. Obstet Gynecol 101: 1112-1116.
- Gerfaud-Valentin M, Hot A, Huissoud C, Durieu I, Broussolle C, et al. (2014) Adult-onset Still's disease and pregnancy: about ten cases and review of the literature. Rheumatol Int 34: 867-871.
- Falkenbach A, Lembcke B, Schneider M, Wigand R, Mulert-Ernst R, et al. (1994) Polyserositis with Adult Still's Disease Onset during Pregnancy. Clin rheumatol 13: 513-517.
- Takeda H, Ling M, Ochi M, Watanabe K (2002) A patient with adult Still's disease with an increased Chlamydia pneumoniae antibody titer. J Infect Chemother 8: 262-265.
- Salamon L, Salamon T, Morovic-Vergles J (2009) Thrombotic microangiopathy in adult-onset Still's disease: case report and review of the literature. Wien Klin Wochenschr 121: 583-588.
- Haram K, Svendsen E, Abildgaard U (2009) The HELLP syndrome: Clinical issues and management. A Review. BMC Pregnancy and Childbirth 9: 8.